These three organizations had a number of characteristics in common:
- Hypercomplexity – extreme variety of components, systems, and levels.
- Tight coupling – reciprocal interdependence across many units and levels.
- Extreme hierarchical differentiation – multiple levels, each with its own elaborate control and regulating mechanisms.
- Large numbers of decision makers in complex communication networks – characterized by redundancy in control and information systems.
- Degree of accountability that does not exist in most organizations – substandard performance or deviations from standard procedures meet with severe adverse consequences.
- High frequency of immediate feedback about decisions.
- Compressed time factors – cycles of major activities are measured in seconds.
- More than one critical outcome that must happen simultaneously – simultaneity signifies both the complexity of operations as well as the inability to withdraw or modify operations decisions.
- Preoccupation with Failure
- Reluctance to Simplify
- Sensitivity to Operations
- Commitment to Resilience
- Deference to Expertise
Today, I want to focus on something called peer review. I am not talking about the "peer review" that occurs when scientists and clinician-investigators submit their study findings for publication in journals. Peer review, in the current context, involves the process by which a physician's quality of care or professional behavior is reviewed by his or her colleagues (i.e., his or her peers) to determine if the quality of care or professional behavior meets certain standards of care. Importantly, the U.S. legal system and other regulatory bodies, such as the Joint Commission, provide certain safeguards to protect the findings of peer review from being used in a malpractice lawsuit.
Peer review is important - who better to review a physician's clinical performance than a fellow physician, someone who knows and fully understands what it is like to practice in a certain clinical environment. I have heard a number of physicians state that if their performance was going to be graded, it better be graded by a physician!
Are their examples of peer review in High Reliability Organizations? Absolutely! As it turns out, virtually every single carrier landing that a pilot in the U.S. Navy makes is graded by a peer - a fellow pilot. The pilot who does the grading is affectionately known as "Paddles" - in the early days of Naval aviation, before the advent of computerized landing systems, pilots were guided on to the aircraft carrier by a fellow pilot (who also graded the landing) using handheld paddles (see the picture below of the character "Beer Barrel" from the classic movie, The Bridges of Toko Ri):

Now that there are computerized landing systems, "Paddles" (the Landing Safety Officer, or LSO)sole function is to grade each pilot's landing - in other words, peer review!

Each landing is graded with a numerical score, and the results for all of the pilots in the squadron are displayed on the "Greenie Board" in the squadron's ready room. The possible results are "OK Pass" (above average, depicted by a green dot with a numerical score of 4.0), "Fair" (average, depicted by a yellow dot with a numerical score of 3.0), "No Grade" (depicted by a "turd brown" dot with a numerical score of 2.0), "Wave Off" (depicted by a red dot with a numerical score of 1.0), or a "Cut" (unsafe pass that did not result in a landing, depicted by a blue dot with a numerical score of 0.0). A "bolter" is a landing attempt in which the tail hook does not catch one of three wires used to "trap" the plane to the deck. As they say in the Navy, "a 'good' landing is one from which you can walk away. A 'great' landing is one after which they can use the plane again!"
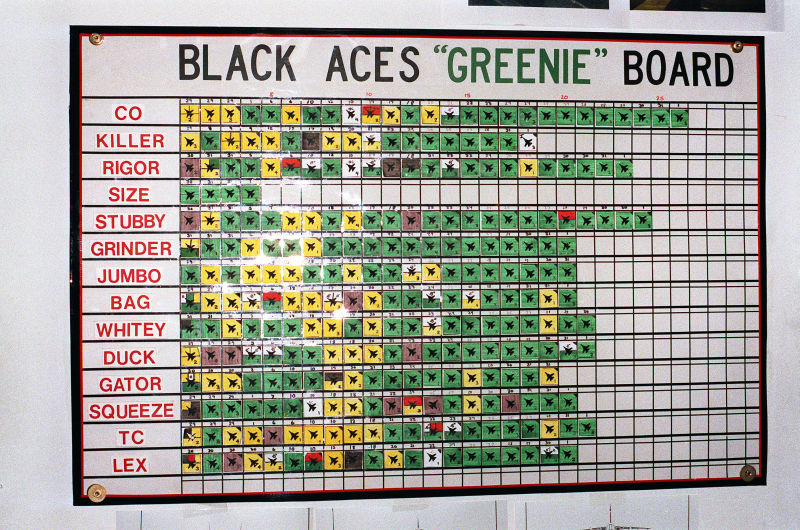
Notice also that these scores and landing grades are completely transparent! Every single pilot, including the commanding officer of the squadron, is listed on the "Greenie Board" for all to see. If someone from another part of the ship happens to visit the squadron ready room, he or she will be able to see the results too. 100% transparency leads to 200% accountability ("I am accountable for my behavior and performance, but I am also accountable for the behavior and performance of my teammates.").
As you think about what happens every single day on an aircraft carrier at sea, think of what we can (and probably should) be doing differently in health care. Many physicians are still reluctant to participate in peer review, or in many cases, think of peer review committees as the "police" or the "bad guys". Not true! If we fail to incorporate peer review into our daily work, then someone else (likely not a peer) will do it for us! Peer review is an important component to achieving high reliability!
No comments:
Post a Comment