Life is all about metaphors and personal stories. I wanted a place to collect random thoughts, musings, and stories about leadership in general and more specifically on leadership and management in health care.
I learned another great story during my recent trip to San Diego. It's a classic from the management literature on conflict resolution and negotiation that was first told nearly 100 years ago by the American social worker Mary Parker Follett. Follett is often called the "Mother of Modern Management" for her contributions to the organizational behavior and organizational theory. In fact, leadership expert Warren Bennis once said about Follett, "Just about everything written today about leadership and organizations comes from Mary Parker Follett's writings and lectures." That's a pretty amazing accolade!
Follett told the story of two sisters who were fighting over an orange. They were both using a different cooking recipe that called for an orange, and neither one wanted to go back to the grocery to purchase another orange. They settled their argument by simply cutting the orange in half. Everything worked out in the end, right? Not so fast! As it turns out, one of the sisters just needed the juice from the orange, while the other just needed the peel for her recipe. Neither recipe worked with just half of an orange. So, in the end, neither sister was able to use the orange.
There is a clear lesson here - the two sisters were using what is called a distributive bargaining technique. Distributive negotiations are what is commonly called a "zero sum game" - one party in the negotiation gains only what the other party loses. However, Mary Parker Follett suggested that the two sisters should have been using an integrative bargaining technique instead. Integrative negotiations occur when the two parties collaborate to find a "win-win" solution to their dispute. Both parties get something out of the deal. Follett may have been the first to describe this technique, though Roger Fisher and William Ury further developed this kind of negotiating strategy in their classic book, Getting to Yes. Imagine what would have happened if the two sisters in our story followed an integrative bargaining approach - the one sister would have all the juice from the orange for her recipe, while the other sister would have all the peel from the orange for hers. Both sisters would have been winners in this case!
In order for the integrative bargaining technique to work, there are a couple of key points to remember. First, you have to always believe that a "win-win" deal is possible. Second, you have to carefully distinguish between interests and positions. Positions are "what they say they want," while interests are "why they want it." A party's interests are their underlying motivations, values, and reasons. During an integrative negotiation, you should focus on the other party's interests rather than their position. Focusing on interests requires patient listening! Try to learn the other party's reasons, motivations, and values. Then try to find a creative solution to meet their needs as well as your own!
Negotiation is an important skill for leaders to learn - they will use it almost every day! Don't be like the two sisters. Find the "win-win" solution. As Mary Parker Follett once said, "There are three ways of dealing with difference: domination, compromise, and integration. By domination only one side gets what it wants; by compromise neither side gets what it wants; by integration we find a way by which both sides may get what they wish."
My February book review is another great adventure story by the American historian and legal scholar, Edward J. Larson (currently the Hugh & Hazel Darling Chair in Law at Pepperdine University) called To the Edges of the Earth: 1909, the Race for the Three Poles, and the Climax of the Age of Exploration. I’ve been going through a "polar explorer" stage, having read several books on Ernest Shackleton's ill-fated voyage to Antarctica and the story of the 1925 diphtheria antitoxin run by dog sled to Nome, Alaska popularized in the animated movie Balto. The "three poles" in the title refers to the North Pole, the South Pole, and the summit of K2, the second highest mountain peak in the world (the so-called "pole of altitude"). The book tells the story of three relatively simultaneous expeditions to the three poles by Prince Luigi Amedeo of Savoy, the Duke of the Abruzzi (K2), American Robert Peary (North Pole), and Ernest Shackleton (South Pole).
Prince Luigi Amedeo, Duke of the Abruzzi, a member of the Italian royal family, was a famous mountaineer who had also tried to reach the North Pole earlier in his career. He mounted an expedition in 1909 to reach the summit of K2, the second highest mountain peak in the world. K2 is located on the border of China and Pakistan and is considered one of the most difficult and dangerous mountains to climb, even now in the present day (about one person dies on the mountain for every four who reach the summit). The Duke was unsuccessful in reaching the summit, claiming that the mountain would never be climbed (notably, the next attempt did not happen until 1938, and the first successful summit did not occur until 1954). Importantly, the Duke established the standard route up this notorious mountain peak.
Shackleton is perhaps more famous for his ill-fated and unsuccessful attempt at crossing the continent of Antarctica in 1914-1917. However, he had also made an unsuccessful attempt at reaching the South Pole in 1909. He did set a new "farthest south" record, and another member of his expedition, Australian Douglas Mawson would reach the south magnetic pole.
Rear Admiral Robert Peary had made a number of unsuccessful attempts to be the first person to travel to the North Pole in the late 19th and early 20th centuries. Peary was accompanied by fellow explorer Matthew Henson on his previous 7 polar expeditions, and it was Henson who was actually the first member of the expedition to reach the geographic North Pole (Henson later published his memoir entitled, A Negro Explorer at the North Pole). After returning to the United States, Peary learned that Dr. Frederick Cook, an American surgeon who had accompanied Peary on an earlier, unsuccessful attempt, had claimed to have reached the North Pole earlier in 1908. A subsequent investigation credited Peary with being the first human to reach the North Pole, though more recent analyses of Peary's logbooks suggest that he too may have failed to reach the actual North Pole. I found it hard to like Peary. He reminded me of a character named Commander McBragg from a cartoon I watched as a child, called "Tennessee Tuxedo and His Tales." He was arrogant, a bit of a braggart, overly obsessed with fame, and unfaithful to his wife and family (he would father a child during the expedition with one of the Inuit women).
The story is more than a history lesson - it is a psychological thriller. Larson weaves all three stories together in such a way that the reader can easily compare and contrast how the three explorers responded to their struggles. Theirs is a story of extreme bravery. Theirs is a story of passion bordering on an obsession leading to insanity. Theirs is a story of the triumph of the human spirit.
All three explorers failed to reach their objective (even though Peary's expedition was initially labeled a success). Regardless, all three men were given a hero's welcome on their return. And that is perhaps why their individual stories resonated with me. There are times when we experience triumph, even when we fail.
Matthew Henson once said, "The path is not easy, the climbing is rugged and hard, but the glory at the end is worthwhile." The journey, in other words, is worth it in the end. Regardless of success or failure.
Shackleton said, "Men are not made from easy victories, but based on great defeats." All of these explorers, each and every one, found victory in their defeat. That is the power of the story in this book.
I heard a very interesting story this past week while attending a medical conference in San Diego, called simply The 18th Camel. There are several different versions of the story on the Internet, but basically the story goes something like this:
There once was a wise Bedouin chief who was traveling across the desert. He came upon an oasis and noticed a small herd of camels with three younger men standing nearby. The three men were arguing with each other and pointing at the camels. The chief walked up to the three younger men and asked, "What is all the commotion about?" The oldest of the three men replied, "Our father has recently died and he left us these seventeen camels. But we cannot agree to divide them between us." "Why is that?" asked the Bedouin chief. One of the other men answered, "You see, sir. Our father left us specific instructions in his will on how to divide up the camels. He wanted one-half of the camels to go to his oldest son, one-third to go to the middle son, and one-ninth to go to the youngest. That's me." The middle son spoke next. "Our problem is that we are unable to follow these instructions. We cannot find a way to follow our dear father's last will." I know what you are thinking, and I thought it too. Why in the world did the father leave specific instructions like this in his will? Did he realize that there is just no way that you can divide the number 17 by one-half, one-third, or one-ninth? Impossible, right? Perhaps he owned more camels when he wrote his will. Oh well, let's see what happens in the rest of the story.
The Bedouin chief thought for a minute. He stroked his beard and then said, "I believe I can help you. How about if I give you the camel I have with me today, and then you will have 18 camels." He turned to the oldest brother, "One-half of 18 camels is nine, and so you are now the proud owner of nine camels." He turned to the middle brother, "One-third of 18 camels is six, and so you now own six camels." Lastly, he turned to the youngest brother. "One-ninth of 18 camels is two. I will give you two of the camels, which is a very good way for a young man to start his life." The wise Bedouin chief looked at all three brothers, who all appeared very happy. "Now, let's count up all of your camels. Nine for the oldest brother, six for the middle brother, and two for the youngest brother. Nine plus six plus two equals seventeen. That leaves the one camel as extra, which I will take back. Farewell."
The wise Bedouin chief got up on his camel and rode away. And everyone was happy. Well, that turned out much different than I had expected! I am not sure how the mathematics works on this, but that is not the point of the story. The moral of the story is this - when faced with a difficult problem, there are times when you have to think creatively to find the solution. It's called "outside of the box" thinking. The best leaders are the ones that can find creative solutions to solve problems, and just like in the story, there are no winners or losers. Leaders can often bring in a fresh perspective to the problem, much like the wise Bedouin chief did. At times, the solution to the problem is right in front of our eyes, and all it takes to solve the problem is a new perspective.
We have been focusing the last several blog posts on what the health care industry can learn from other high reliability organizations, specifically U.S. Navy aircraft carrier flight operations, to improve the overall quality of care delivery. We have covered topics such as peer review,color-coding a specific functional team's uniforms,FOD walks, and the Officer of the Deck (OOD). Today, I want to go back to something I mentioned in an earlier post - specifically, the importance of leadership. In talking about the Solutions for Patient Safety network, I mentioned that one of the fundamental tenets of safety in this network of over 135 children's hospitals is the direct involvement of both the CEO and the Board in safety. The CEO and Board must adopt a "Buck Stops Here" mentality when it comes to safety. As it turns out, leadership definitely matters.
Other high reliability organizations recognize the importance of leadership too. High reliability leadership principles are fundamental to high reliability operations! That is certainly true for U.S. Navy aircraft carriers. There is something very unique, however, about the commanding officer (CO) of an aircraft carrier. The CO of an aircraft carrier always comes from the ranks of Navy pilots. Pilots can be easily recognized by the fact that they wear brown shoes (all other officers wear black shoes) and wear gold wings above their left shirt pocket. So, every CO of an aircraft carrier wears brown shoes and gold wings. They typically have between 20-25 years of flying experience with incrementally increased leadership responsibilities, including command of a carrier-based squadron. In addition, prior to becoming the CO, a pilot must complete training at Navy Nuclear Power School (a six month course with a heavy focus on physics, engineering, and mathematics), followed by six additional months of Navy Nuclear Power qualification. After serving a tour as the Executive Officer (XO) of an aircraft carrier, the successful candidate would then serve a tour as the commanding officer (CO) of a surface ship, usually a Marine transport ship, oiler, or supply ship.
Why does the Navy insist (it's actually legally proscribed) on having experienced pilots in command of its aircraft carriers? One word - culture. Only a pilot can truly appreciate the intense demands of flying and landing an aircraft on the deck of a pitching and rolling ship in the middle of the ocean. It's all about setting the right expectations and achieving operational excellence through a culture of high reliability. Navy pilots are unique individuals - having a fellow pilot serve as their leader brings that unique culture to the rest of the ship.
So, the next logical question. If hospitals are looking to learn from other high reliability organizations, such as U.S. Navy aircraft carriers, should hospitals require that their CEO (the civilian counterpart of the aircraft carrier CO) come from the clinical ranks? There are certainly a few excellent health care organizations that have this requirement (I am thinking, in particular, of the Mayo Clinic and the Cleveland Clinic, two health care organizations that are perennially listed at the top of the nation's best hospitals). I am not suggesting anything new - there are studies showing that hospitals that are run by either physician or nurse CEO's have better quality, better patient experience, and lower costs than those that are run by non-clinician CEO's. According to a study by Amanda Goodall, hospitals that are led by physician or nurse CEO's have quality metric scores as much as 25% higher than those led by non-clinician CEO's. Unfortunately, fewer hospitals today are led by clinician CEO's (according to a 2009 study published in the journal Academic Medicine, only 235 of nearly 6,500 hospitals across the United States were led by physician CEO's).
Most clinicians don't have the experience of managing a large organization or a big budget. However, more clinicians are taking graduate programs in health care administration or business administration than ever before. With gradually increasing experience, akin to the education, training, and experiences that pilots go through, there is absolutely no reason why clinicians can't get the requisite experience to run even large hospitals. With a similar training pathway, physicians and nurses can get just enough financial experience to work with an experienced Chief Financial Officer to lead a health care organization. After all, there is no way that an aircraft carrier CO will have as much experience driving a ship as a Naval Surface Warfare officer who became a CO after rising through the ranks of the surface Navy (destroyers, cruisers, frigates, amphibious assault ships, etc). However, that aircraft carrier CO has enough experience, especially when paired with a team of surface warfare operators, that he (as of today, there have been no female CO's of aircraft carriers, though that will likely change in the very near future) can do the job and perform to the standards of a high reliability organization!
It's a lot to think about. But the overall mission of health care is still focused on patient care. Who better to lead a hospital than someone who has dedicated their lives to direct patient care?
The singer-songwriter, author, and Nobel Laureate Bob Dylan wrote a song called "All Along the Watchtower" that has been covered by a number of artists across several different musical genres, most famously by the artist Jimi Hendrix (Hendrix's version is listed at number 47 on Rolling Stone magazine's 500 Greatest Songs of All Time). The song is packed with meaning, but beyond that it's just a really great song!
According to Merriam-Webster's online dictionary, a watchtower is a tower for a lookout, built to specifically create an elevated observation point from which a sentinel or guard may observe the surrounding area. The sentinel's main job is to prevent a surprise attack - in other words, to protect and keep everyone else safe. Note also that the Joint Commission uses the word in their classification system, defining a "sentinel event" as "any unanticipated event in a healthcare setting resulting in the death or serious physical or psychological injury to a patient, not related to the natural course of the patient's illness." In other words, a "sentinel event" is an early warning indicator of a (usually) much bigger safety issue in an organization.
I would like to keep with this theme and build upon our discussion of high reliability organizations, and more specifically, U.S. Navy aircraft carrier flight operations (see the last few posts). Specifically, most high reliability organizations have adopted this watchtower or sentinel concept. For example, the Officer of the Deck, or OOD is an individual on every ship who serves as a direct representative of the ship's commanding officer and who is given certain responsibilities, authority, and oversight to maintain normal, safe operations while a ship is underway at sea or in port. While in port, the OOD is stationed on the quarterdeck (the entry point to the ship). At sea, the OOD is stationed on the bridge and is in charge of navigation and safety of the ship (until relieved of these duties by the commanding officer or his/her designee). The Naval Institute Press publishes a book called the Watch Officer's Guide which provides further details on these roles and responsibilities. Importantly, several individuals on the ship will serve as the OOD in such a way that there is always an OOD either on the quarterdeck (while in port) or the bridge (while underway at sea) for every hour of the day.
So the next logical question is this - do hospitals, in their quest to become high reliability organizations, have a similar role to the OOD? Interestingly enough, at least one hospital (my own) has borrowed this concept in developing a role called the Safety Officer of the Day. The Safety Officer of the Day (SOD) is a relatively experienced physician (we currently have two surgeons, one anesthesiologist, two emergency medicine physicians, and three to four pediatric subspecialists who share this role) who have the authority and responsibility to assist frontline physicians and nurses with mitigating any safety and/or communication concerns on our inpatient units. These individuals generally serve as the SOD for a week-long block and attend our inpatient bed huddles (two per day) and daily operations briefings (every morning), where they role model and reinforce key safety behaviors, provide coaching, and escalate any concerns, when appropriate. The SOD works closely with the Manager, Patient Services (MPS), an experienced nurse who is tasked with patient flow, safety, and nurse staffing throughout the day. The SOD/MPS dyad is an important part of our overall patient safety plan, which over time has resulted in a significant improvement in situation awareness, decreased code events, and timely and appropriate transfer to the Pediatric Intensive Care Unit.
There are certainly other ways to model the OOD concept in health care organizations, but we believe that the SOD/MPS dyad is one of the most important design changes that we have implemented to improve the early recognition and treatment of patients who are at risk of clinical deterioration in the inpatient environment. The SOD serves as a sentinel in our watchtower to help keep our patients safe!
I want to stay with our theme on High Reliability Organizations for just a little while longer. There is another concept used in Navy flight operations that I think we can learn a lot from in health care. Hopefully, I convinced you in my last post that the flight deck of a Navy aircraft carrier is a very dangerous place. If you don't believe me still, check out this video of a member of the flight deck crew getting sucked up into the jet engine of an A-6 Intruder several years ago. Remarkably, the sailor escaped with only minor non-life-threatening injuries. He was lucky! But it's not just humans that can get sucked up into an aircraft engine. Any piece of debris can cause a lot of damage to an airplane's engine, potentially causing the airplane to crash.
An article in the Navy Times estimated that the engine of an F/A-18C Hornet costs around $1.5 million to replace if it is damaged by random debris on the flight deck. Engine replacement costs for the more advanced fighter, the F/A-18F Super Hornet costs around $3.5 million to replace. And that assumes that a spare engine is readily available (they usually are), which may not always be the case when an aircraft carrier is out in the middle of the ocean and far from home.
Given the costs associated with the possible loss of an airplane, as well as the potential risk to the life of the pilot or other crew members on the flight deck if an airplane crashed due to so-called "Foreign Object Damage" (commonly abbreviated as FOD), before any airplane engine is started on the flight deck, the entire flight deck crew conducts what is known as a FOD walk. FOD walks are considered "all-hands" evolutions - meaning almost everyone participates!
If a sailor finds an object on the flight deck, no matter how small, he or she will hold it up in the air and continue to look for more objects. All objects are then brought before a quality assurance team (on some aircraft carriers, the Commanding Officer, Air Wing Commander, and various Department Heads comprise the quality assurance team) to review the list of objects that were found, as well as the location where they were found. The information is then used to make improvements.
Can you imagine a hospital CEO (the equivalent of a Commanding Officer) getting involved in a safety exercise such as a FOD walk? It actually does happen! There is a large network of children's hospitals, called the Solutions for Patient Safety network (the network started with the 8 children's hospitals in the state of Ohio and now comprises over 135 children's hospitals in the U.S. and Canada) focused on eliminating patient harm, largely through many of the techniques borrowed from High Reliability Organizations, such as Navy aircraft carriers. One of the fundamental tenets for improving patient safety has been to involve the hospital CEO and the Board of Trustees in patient safety. These hospitals, and other High Reliability Organizations have found that leadership matters - executive level leadership and oversight of patient safety is critical to reducing the harm that occurs to patients in the hospital setting. The CEO and Board of participating hospitals in the SPS network sign an agreement that they will take ownership of patient safety in their organization and that they will not compete on safety with other hospitals. SPS estimates that more than 9,000 children have been spared harm since 2012, while avoiding over $148.5 million in health care spending at the same time!
What is our FOD walk in the health care setting? Well, I can think of a couple. The SPS Network has implemented a number of "bundles" directed at reducing, and in some cases, eliminating, hospital-acquired conditions, including pressure ulcers ("bed sores"), central line infections, ventilator-associated pneumonias, urinary tract infections, and medication errors. Each bundle consists of a relatively small number of evidence-based practices that, when performed religiously every day, reduce the rate of these hospital-acquired conditions. If a hospital wants to lower the rate of a specific hospital-acquired condition, all they have to do is increase the compliance with the relevant bundle (there is, of course, a little more to it than that, but you get the idea). Maintaining bundle compliance is our version of the FOD walk!
If you don't believe me, check out an article by the folks in the Pediatric Intensive Care Unit (PICU) at C.S. Mott Children's Hospital. Apparently, the PICU team there increased and maintained their unit's ventilator-associated pneumonia bundle compliance from <50% (in other words, less than half of the time, the specific elements to reduce the risk of pneumonia were actually followed) to well over 75% over the course of 12 months. The increase in bundle compliance was associated with a dramatic reduction in ventilator-associated pneumonia. The leaders of the PICU found out that the physicians, nurses, and allied health staff felt that the checklist used to monitor bundle compliance was overly burdensome, so they stopped monitoring it. After all, they had nearly eliminated ventilator-associated pneumonia and were setting their sight on other improvement projects. During the next 4 months after stopping the monitoring, the ventilator-associated pneumonia rate spiked back up and rose to their previous level. So, they re-initiated bundle compliance monitoring and the rate returned to near zero.
What's going on here? In my mind, this (bundle compliance monitoring) is our FOD walk! No matter what we do, patients in the hospital will always be at risk of developing one or more of these hospital-acquired conditions. That's a fact of life. We can dramatically lower the risk, but we will never be able to completely eliminate that risk. But we can eliminate the hospital-acquired conditions. So, in order to maintain vigilance, as long as patients are at risk, we have to monitor bundle compliance. How else will we know if we are doing the right thing?
I guess it all comes to down to this. If you want to improve safety, take a FOD walk!
There is a really cool museum in San Diego, California called the USS Midway Museum, located in the downtown area at Navy Pier. The museum is housed (and mainly consists of) the aircraft carrier, USS Midway, which was in active service from 1945 to 1992. One of the things you may see at the museum are manikins dressed up in the various Navy uniforms that you would have seen on the aircraft carrier while it was in active service. There really is a rainbow of colors! Keeping with our theme on High Reliability Organizations and what we can learn from aircraft carrier flight operations (one of the three original HRO prototypes), today I would like to discuss a little more about this rainbow of colors.
All of the more than 5,500 crew members on a United States Navy aircraft carrier really exist to perform one duty - put aircraft (planes and helicopters) into the air and safely recover them after they leave the flight deck. Many of these crew members actually work on the busy flight deck. It's really something to watch (there are plenty of videos online - here is one that is called "Controlled Chaos"). Each individual crew member has his or her special role, and the role is designated by the color of the shirt that he or she wears (see the pictures below).
Here is a quick guide to the color-coded jerseys on an aircraft carrier from the U.S. Navy's website:
Purple: Aviation Fuels (nickname: "Grapes")
Blue: Plane Handlers, Aircraft Elevator Operators, Tractor Drivers, Messengers and Phone Talkers
Green: Catapult and Arresting Gear Crews, Air Wing Maintenance Personnel, Cargo Handlers
Brown: Air Wing Plane Captains, Air Wing Line Leading Petty Officers
White: Air Wing Quality Control, Inspectors, Safety Observers, Medical Personnel, Landing Signal Officer, Liquid Oxygen Crews
Fairly impressive, right? Each job category is grouped into a larger category of functions (e.g., individuals wearing white jerseys generally involve medical and safety related functions). It's all very systematic and highly organized, all of which contribute significantly to the "controlled chaos" of flight deck operations.
When you consider all of the different job categories and types of health care providers working in the hospital setting, it seems logical to ask whether hospitals have adopted a similar system of color-coding. It turns out, I know of at least one health care organization that color codes the scrubs of everyone working in the hospital. It's a specialty hospital (basically taking care of adults with acute heart disease) that I had an opportunity to visit a few years ago. As I was walking around, I noticed a sign posted on every patient room that described their own "rainbow of colors" - here is a picture:
Pretty interesting, right?!?! One of the common complaints I hear from patients and families is that they never know the exact role of the individuals that enter their rooms. Some hospitals, including ours, tried to address this by wearing an attachment on our name badge that states our role (e.g., attending physician, fellow, resident, nurse, respiratory therapist, social worker, etc). The cardiac hospital I visited solved this issue by having everyone wear a different color of scrubs.
I asked several of the workers whether they liked the different color of scrubs. They actually said that they wore their different colors with pride. If you look at the sign carefully, you will also notice that physicians aren't mentioned. I asked about that too. Most of the physicians that I spoke with said that they wore a white lab coat (none of the physicians were employed directly by the hospital), but I did think that it was a miss not to include them (or for that matter, nurse practitioners or physician assistants) on the list.
It's an interesting thought. I would love to hear what the patients and families think, as well as hearing more from the hospital staff as well. The parallel with what the U.S. Navy is doing with carrier flight operations is also intriguing.
The patient safety movement in health care has borrowed heavily from lessons learned in both commercial and military aviation for the past several years. For example, one of the earliest descriptions of so-called High Reliability Organizations (defined as organizations that operate in complex, dangerous environments for extended periods of time without experiencing serious accidents or catastrophic events) studied three different organizations - a nuclear power plant owned by Pacific Gas & Electric Company (the Diablo Canyon Power Plant on the coast of California), the Federal Aviation Authority's air traffic control operations, and flight operations on an United States Navy aircraft carrier (the U.S.S. Carl Vinson).
Hypercomplexity – extreme variety of components, systems, and levels.
Tight coupling – reciprocal interdependence across many units and levels.
Extreme hierarchical differentiation – multiple levels, each with its own elaborate control and regulating mechanisms.
Large numbers of decision makers in complex communication networks – characterized by redundancy in control and information systems.
Degree of accountability that does not exist in most organizations – substandard performance or deviations from standard procedures meet with severe adverse consequences.
High frequency of immediate feedback about decisions.
Compressed time factors – cycles of major activities are measured in seconds.
More than one critical outcome that must happen simultaneously – simultaneity signifies both the complexity of operations as well as the inability to withdraw or modify operations decisions.
Importantly, while many organizations exhibit one or a few of these characteristics, high reliability organizations exhibit all of them simultaneously! Also, these characteristics defined why, but not necessarily how these organizations were high reliability organizations. In other words, these characteristics defined the complex, dangerous environments in which these organizations operated. How these organizations responded to these factors determined how they became high reliability organizations. As I have discussed in a number of previous posts, the following five characteristics defined the "how":
As it turns out, while these are the essential and defining characteristics of High Reliability Organizations, these organizations do a lot more to reduce the likelihood of a serious accident (or at least limit the consequences of the serious accident). Here is where those of us in the health care industry can learn a lot more from U.S. Navy flight operations at sea.
Today, I want to focus on something called peer review. I am not talking about the "peer review" that occurs when scientists and clinician-investigators submit their study findings for publication in journals. Peer review, in the current context, involves the process by which a physician's quality of care or professional behavior is reviewed by his or her colleagues (i.e., his or her peers) to determine if the quality of care or professional behavior meets certain standards of care. Importantly, the U.S. legal system and other regulatory bodies, such as the Joint Commission, provide certain safeguards to protect the findings of peer review from being used in a malpractice lawsuit.
Peer review is important - who better to review a physician's clinical performance than a fellow physician, someone who knows and fully understands what it is like to practice in a certain clinical environment. I have heard a number of physicians state that if their performance was going to be graded, it better be graded by a physician!
Are their examples of peer review in High Reliability Organizations? Absolutely! As it turns out, virtually every single carrier landing that a pilot in the U.S. Navy makes is graded by a peer - a fellow pilot. The pilot who does the grading is affectionately known as "Paddles" - in the early days of Naval aviation, before the advent of computerized landing systems, pilots were guided on to the aircraft carrier by a fellow pilot (who also graded the landing) using handheld paddles (see the picture below of the character "Beer Barrel" from the classic movie, The Bridges of Toko Ri):
Now that there are computerized landing systems, "Paddles" (the Landing Safety Officer, or LSO)sole function is to grade each pilot's landing - in other words, peer review!
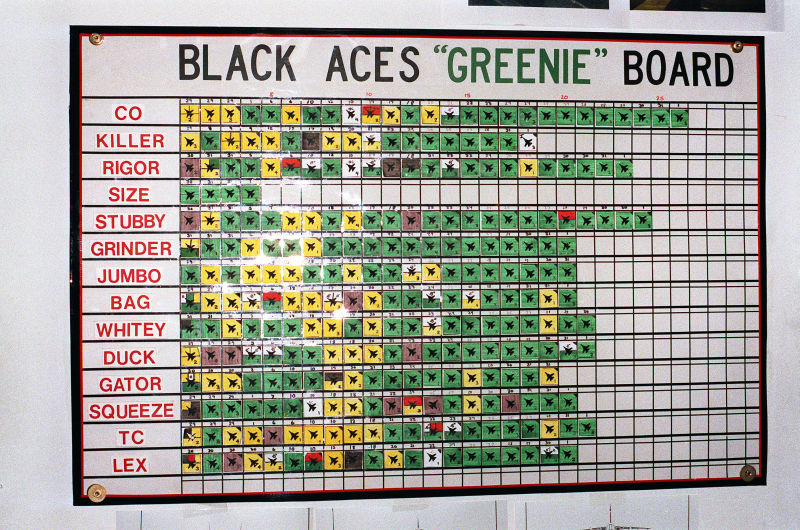
Each landing is graded with a numerical score, and the results for all of the pilots in the squadron are displayed on the "Greenie Board" in the squadron's ready room. The possible results are "OK Pass" (above average, depicted by a green dot with a numerical score of 4.0), "Fair" (average, depicted by a yellow dot with a numerical score of 3.0), "No Grade" (depicted by a "turd brown" dot with a numerical score of 2.0), "Wave Off" (depicted by a red dot with a numerical score of 1.0), or a "Cut" (unsafe pass that did not result in a landing, depicted by a blue dot with a numerical score of 0.0). A "bolter" is a landing attempt in which the tail hook does not catch one of three wires used to "trap" the plane to the deck. As they say in the Navy, "a 'good' landing is one from which you can walk away. A 'great' landing is one after which they can use the plane again!"
Notice also that these scores and landing grades are completely transparent! Every single pilot, including the commanding officer of the squadron, is listed on the "Greenie Board" for all to see. If someone from another part of the ship happens to visit the squadron ready room, he or she will be able to see the results too. 100% transparency leads to 200% accountability ("I am accountable for my behavior and performance, but I am also accountable for the behavior and performance of my teammates.").
As you think about what happens every single day on an aircraft carrier at sea, think of what we can (and probably should) be doing differently in health care. Many physicians are still reluctant to participate in peer review, or in many cases, think of peer review committees as the "police" or the "bad guys". Not true! If we fail to incorporate peer review into our daily work, then someone else (likely not a peer) will do it for us! Peer review is an important component to achieving high reliability!
Last night, for the second time in 100 days (98 days to be exact), a professional sports team from the city of Boston defeated a professional sports team from the city of Los Angeles for a world championship. In other words, the NFL football team that I hate the most (which also happens to be the NFL football team that I admire and respect the most) - the New England Patriots won their record-tying sixth Super Bowl championship, beating the Los Angeles Rams in Super Bowl LIII by a score of 13-3. Just in case you are wondering, 98 days before the Patriots beat the Rams, the Boston Red Sox defeated the Los Angeles Dodgers in the 2018 World Series.
It has been an amazing run for the Patriots. Whenever sports commentators talk about the Patriots, they use terms like dynasty and historic. The franchise has played in more Super Bowls (eleven) than any other team, winning six of them and losing five. Head Coach Bill Belichick and quarterback Tom Brady have won all six of those Super Bowls, winning their first in 2001. They have played (and lost) in three others, losing the New York Giants twice and the Philadelphia Eagles once (last year). That makes a total of nine Super Bowls that Coach Belichick and Brady have coaches and played in, respectively, together! Tom Brady has now won more Super Bowls than any other player in the history of the NFL. Coach Belichick already held the record for the most Super Bowl wins as a head coach, but as of last night he became the oldest head coach in the history of the NFL to win the Super Bowl. He still has fewer overall NFL league championships than Coach George Halas of the Chicago Bears (7 total wins), though there are many that believe that he will surpass even legendary Coach Halas in the next couple of years. He has no plans on retiring soon!
One could easily argue (and many have) that Coach Belichick will one day retire as the greatest head coach in the history of the NFL, and almost everyone believes that Tom Brady is already there as the greatest quarterback to ever play in the NFL. These two individuals are the constants. So, how do the continue to win, year after year? What is the secret to their success? In a word? Culture.
I have written about the Patriots winning culture before (see my previous posts, "The Patriot Way" from February 5, 2017 and The Patriot Way Redux from January 7, 2018). I would ask, "What more evidence do you need to convince you?" Remember, Coach Belichick and Tom Brady are really the only two (as far as I know) consistencies between their first Super Bowl win together in 2001 and their sixth win last night. There is no question that the Patriots have a talented roster, year in and year out. However, one could argue that the Los Angeles Rams had more talent last night than the Patriots. One could also argue that the Patriots rarely are the most talented team in the NFL, yet they continue to find ways to win, over and over. It all comes down to culture.
Here are two really great examples of what I am talking about. A few weeks ago, an article appeared on Inc.com entitled "Tom Brady Says the Same 4 Words to Every New Player on the New England Patriots, and It's Pure Genius". The story first appeared in an article by Adam Kilgore of the Washington Post. Basically, whenever a new player walks into the locker room at the start of the year on the first day of practice, future Hall of Fame quarterback, the GOAT ("Greatest of All-Time"), and the player who has now won more Super Bowls than anyone, EVER, walks up and says, "Hi. I'm Tom Brady." In other words, Tom Brady, who at age 41 is older than every other player in the locker room, treats every new player as an equal. There are no superstars. No one gets special treatment. Here, on the Patriots roster, everyone is the same. Culture.
The next article also comes from the Washington Post and is entitled, Bill Belichick makes Tom Brady study punt coverages. It helps explain the Patriot's reign. Coach Belichick continues to emphasize special teams play (kicking and punting). Adam Kilgore says the following about Belichick, "He treats special teams not as something that happens between offense and defense, but as a full third of the game." He goes on to say that Belichick, "uses them to promote solidarity. He demands correct execution down to excruciating detail." Every week, the team does a full session studying special teams film. And when I say "the team", I mean the whole team. Everyone, including quarterback Tom Brady, spends time watching game film of special teams play. Does Brady complain? Absolutely not. Belichick sends a clear message that he expects everyone to know the game plan from start to finish and that all three phases of the game (offense, defense, and special teams) need to be played flawlessly if the team has any chance at winning. Brady sends a clear message that no one is more important than anyone else. Here, on the Patriots, everyone contributes and no one gets special treatment. Everyone is the same. Culture.
It's really very cool when you think about it. Unfortunately, it has to be the New England Patriots. And too bad for the city of Los Angeles. Last night makes it twice.
Last year on February 3rd, I wrote a post entitled "Do we need a National Women Physician's Day"? The question was rhetorical in nature, as I strongly support (as did the post) having a separate National Women Physician's Day. The day is celebrated on the birthdate of Dr. Elizabeth Blackwell, the first woman to receive a medical degree in the United States of America. Dr. Blackwell once said: "If society will not admit of a woman's free development, then society must be remodeled."
Dr. Blackwell's statement is absolutely true. We should (and we are) remodeling society, slowly but surely. We've made a lot of progress over the years, but we have so far to go. Two examples from this past year are notable.
First, in September of last year, a physician in Dallas, Texas became quite famous for a statement that he made in the Dallas Medical Journal. The journal had asked several physicians to comment on the gender pay gap (a study published in 2016 in JAMA Internal Medicine found that women physicians earn, on average, 8% less than their male counterparts, while a survey conducted on Doximity found that women earned almost 28% less than their male counterparts in 2017) in medicine. Dr. Gary Tigges, an internal medicine physician practicing in Dallas, stated that, "Yes, there is a pay gap. Female physicians do not work as hard and do not see as many patients as male physicians. This is because they choose to, or they simply don’t want to be rushed, or they want to work the long hours. Most of the time, their priority is something else… family, social, whatever." He went on to say, "Nothing needs to be ‘done’ about this unless female physicians actually want to work harder and put in the hours. If not, they should be paid less. That is fair.” Dr. Tigges later offered an apology, but only after he was forced to resign and only after he was absolutely blistered (deservedly so) on social media.
Second, a group of (male) investigators in Basel, Switzerland published a study in the journal, Critical Care Medicine that compared the simulated outcomes from a cardiopulmonary arrest when the resuscitation team was led by a male versus a female physician. In this study, which did not involve actual, real patients (and involved only medical students, who never actually lead resuscitation teams in real life scenarios), female-led teams showed less "hands on time" and longer delays to initiate chest compressions (both of which impact outcomes) compared to male-led teams. The study's investigators wrote, "The management of a cardiac arrest situation by a team of first responders is a highly time-critical emergency event that requires short and precisely verbalized commands by a determined leader, rather than a focus on social relationships or affective issues. A cardiac arrest situation should therefore favor males as primary leaders. Our results are in line with this conclusion." A large, retrospective study was published just this month in the same journal that looked at the outcomes in 1,082 adult cardiopulmonary arrests that occurred in two hospitals. The odds of survival (i.e., actual outcomes rather than surrogate outcomes, such as "hands on time" and "time to initiate chest compressions") were significantly improved when female physicians led the resuscitation team.
We clearly have some work to do. First, there is a gender pay gap that we have to address. Does the opinion of one physician that women physicians don't get paid as much because they don't work as hard as their male colleagues mean that all male physicians feel this way? Absolutely not. But the fact that one physician felt justified in making this kind of claim in such a public way is illustrative of part of the problem that women physicians face. Second, the fact that a group of investigators felt justified in making a statement that resuscitation teams should always be led by a male physician, based on a study involving simulated cardiopulmonary arrests managed by individuals with limited training and experience is also noteworthy. The study was the focus of conversation at a number of national meetings, and representatives from the journal stated that they published the paper as written in order to generate discussion. Mission accomplished. The fact remains that studies involving real patients and real outcomes continue to show superior outcomes when female physicians are involved.
So, I ask again. Do we need a National Women Physician's Day? Until the gender pay gap is eliminated, and when female physicians receive the respect and recognition to which they are entitled, I say absolutely and unequivocally yes.
Thank you again to Dr. Elizabeth Blackwell for leading the way. And to all of my female physician colleagues, enjoy your day!
Jackie Robinson, the first Black American to play in Major League Baseball when the Brooklyn Dodgers started him at first base on April 15, 1947, would have celebrated his 100th birthday just a few days ago, on January 31, 2019. Aside from that incredible accomplishment (more on that later), Mr. Robinson was an incredible baseball player. During his 10-year career playing for the Dodgers, Robinson won the Rookie of the Year Award in 1947, was named an All-Star for six consecutive seasons from 1949 through 1954, won the National League Most Valuable Player Award in 1948, and played in six World Series (winning it all in 1955), and was inducted into the Professional Baseball Hall of Fame in 1962. One can only imagine how his career would have gone if he had played more than 10 years, as many professional baseball players do today. After his death in 1972, Robinson was posthumously awarded the Congressional Gold Medal and the Presidential Medal of Freedom. In 1997, Major League Baseball retired his jersey number "42" on every professional baseball team - no one playing on any team will ever wear the number "42" ever again (except on Jackie Robinson Day, celebrated every year on April 15th, the day that he made his Major League debut, when every single player on every single team wears that number)!
There is a well known story, perhaps made famous by the 2013 movie about Jackie Robinson, "42" starring Chadwick Boseman that involves both Robinson and the Hall of Fame Dodgers shortstop Pee Wee Reese. The incident reportedly occurred at Crosley Field, home (at that time) of the Cincinnati Reds and the southernmost (again, at that time) professional baseball team playing in the major leagues on June 21, 1947. It was Robinson's first game playing in Cincinnati. The crowd was yelling vicious and hateful racist slurs against Robinson as the Dodgers took the field. The crowd was also yelling at Reese, who had grown up in the South near Louisville, Kentucky, calling him "Traitor!" and "Carpetbagger!" Reese finally walks over across the infield towards Robinson, who is playing first base. The scene, as depicted in the movie goes like this:
Robinson: "What's up?"
Reese: "They can say what they want; we're here to play baseball."
Robinson: "Just a bunch of crackpots still fighting the Civil War."
Reese: "Hell, we'd have won that son of a gun if the cornstalks had held out. We just ran out of ammunition."
Robinson (laughing): "Better luck next time, Pee Wee."
Pee Wee Reese puts his arm around Jackie Robinson.
Reese: "Ain't gonna be a next time. All we got is right now. This right here. Know what I mean?"
Crowd looks shocked and horrified that Reese has his arm around Robinson.
Reese: "Thank you, Jackie."
Robinson: "What're you thanking me for?"
Reese: "I've got family here from Louisville up there somewhere. I need them to see who I am."
It's a great scene. There is a statue in Brooklyn showing Reese with his arm around Robinson.
There's even a plaque on the former Crosley Field site (now the site of the City Gospel Mission) in Cincinnati, Ohio at the exact spot where "the embrace" is said to have occurred. The problem is that the event probably never occurred, at least how the scene was depicted in the movie. There are no known photographs of the event, nor are there any published news stories found describing what had happened. Neither Pee Wee Reese nor Jackie Robinson could pinpoint the actual event, but both described something like it. It probably occurred in 1948 (Robinson's second season), and may not have even happened in Cincinnati.
Regardless, it is a great story. Jackie Robinson's widow, Rachel Robinson, was present at the statue's dedication in Brooklyn in 2005. She said, "It's a historic symbol of a wonderful legacy of friendship, of teamwork, of courage -- of a lot of things we hope we will be able to pass on to young people. And we hope they will be motivated by it, be inspired by it and think about what it would be like to stand up, dare to challenge the status quo and find a friend there who will come over and support you."
Regardless of the exact details of "the embrace", no truer words have been spoken. It is a timeless story of friendship, teamwork, and courage. And it is a story that we need to hear, over and over, today.